
MS2.2 FFM Case Review 2
Published:
- 1. Palpitations in a post-menopausal woman [1]
- 2. Chronic nausea and vomiting in a young woman [3]
- References
1. Palpitations in a post-menopausal woman [1]
Chief complaint
Heart palpitations and high blood pressure for the past 2-3 hours.
History of present illness
X is a 5x year old female who presents to urgent care for heart palpitations and a high blood pressure, measured 160/110 mmHg this afternoon during a routine dental appointment for dental cleaning. Her palpitations began 3 weeks ago. She describes them as an uncomfortable, ‘pounding’ sensation in her chest that radiates to her neck and sometimes her head. Episodes occur intermittently and may last for hours. Over the past 3 weeks, she has noted an increase in the frequency of episodes, especially when working. She attributes this to increased stress at her job. There are no notable palliating factors. She also notes shortness of breath on exertion; her office at work is on the 12th floor, and she has recently had to pause every 5 flights of stairs, whereas she previously could climb all 12 flights without pausing.
She denies chest pain, syncope, light-headedness, sweating, headaches, vision changes, swelling, or weakness.
- Structural vs. ischemic cardiac causes
- Hypoglycemia = neurogenic (early) vs. neuroglycopenic (late), e.g. shaking, sweating, anxiety, hunger, nausea, tingling > confusion, weakness, vision changes, slurred speech, irritability, seizures
- GAD, panic attack = shortness of breath, nervousness, gastrointestinal upset, muscle aches, tension, and insomnia
- Hyperventilation (anxiety) = dyspnea, dizziness, tingling in the hands/face
Medical history is significant for dyslipidemia, for which she takes a statin, and pre-diabetes mellitus. There is no personal or family history of heart attack or stroke. Her mother was diagnosed with atrial fibrillation at age 61, managed with a pacemaker.
She drinks half a cup of coffee a day. She has never smoked and does not drink alcohol. She denies use of recreational drugs.
She is concerned that her symptoms may be due to stress and/or hormonal changes due to menopause. She denies hirsutism, vaginal dryness/itching, dyspareunia, bone pain, or fractures. Although she denies sleep changes, she notes that her palpitations sometimes make it difficult for her to lie down, leading to prolonged sleep latency. Otherwise, her palpitations do not disrupt her sleep and her sleep duration and quality are normal.
Objective
- General: awake, alert, no apparent distress
- Vitals: BP 160/110 mmHg measured on admission; HR regular 86 bpm
- Respiratory: good air entry bilaterally; no finger clubbing
- CV: normal S1 and S2 heart sounds, no murmurs; normal capillary refill; radial and brachial pulses are 2+
- HEENT: thyroid is not enlarged; no exophthalmos
- ECG: sinus rhythm with incomplete RBBB and non-specific ST-T changes (complicated by movement artefacts)
Assessment/Plan
Assessment
X is a 5x year old female with heart palpitations and normal ECG suggests:
- paroxysmal atrial fibrillation
- paroxysmal supraventricular tachycardia (PSVT)
- sinus tachycardia with underlying cardiac dysfunction
- hyperthyroidism
- secondary hypertension
Critical diagnoses include: acute coronary syndrome / ischemic heart disease; heart failure; and pheochromocytoma.
Problem list and plan:
Counsel regarding red flags for urgent evaluation:
- syncope or presyncope
- sustained palpitations with hemodynamic instability
- chest pain or ischemic symptoms (syncope, angina, dyspnea)
worsening exertional symptoms
- Labs
- CBC for anemia (high-output state may cause palpitations)
- Extended electrolytes (Ca, Mg, K)
- creatinine/eGFR
- glucose
- TSH and free T4 (hyperthyroidism)
- Lipid panel and HbA1c for CVD risk
- urinalysis with urine ACR for end organ damage in diabetes/hypertension
- BNP if HF suspected
- Cardiac rhythm monitoring: 24-H Holter ECG
- Echocardiography for structural heart disease, diastolic dysfunction, valvular disease, and LV function
- Hypertension:
- Repeat BP measurement in office setting
- Consider home BP monitoring or ambulatory BP monitoring
- If hypertension is diagnosed, initiate anti-HTN therapy [2]:
- Thiazides, e.g. HCTZ: Monitor for hyponatremia and hypokalemia, increased glucose, uric acid, and calcium levels. Monitor patients with history of acute gout unless patient is on uric acid-lowering therapy.
- ACEi, e.g. captopril: There is an increased risk of hyperkalemia, especially in patients with CKD or in those on K+ supplements or K+-sparing drugs. There is a risk of acute renal failure in patients with severe bilateral renal artery stenosis. Do not use if patient has history of angioedema with ACEi.
- ARBs, e.g. candesartan
- DHP CCBs, e.g. diltiazem: Avoid routine use with beta blockers because of increased risk of bradycardia and heart block. Do not use in HFrEF.
- Screening for secondary hypertension:
- Primary aldosteronism: plasma aldosterone/renin ratio
- Pheochromocytoma: 24-H urinary fractionated metanephrines
- Additional tests:
- Stress testing for persistent ischemic symptoms or palpitations that occur specifically with exertion
- Sleep evaluation (STOP-BANG)
- Confirm statin type and dose
- Follow-up
- Counsel about red-flag symptoms (see above)
- Review ambulatory monitoring results and lab studies in 2-4 weeks
- Cardiology referral if arrhythmia, structural heart disease, or progressive symptoms
- Reassess BP control and symptoms after initiating therapy
| CAUSE | NATURE OF PATIENT | NATURE OF SYMPTOMS | ASSOCIATED SYMPTOMS | PRECIPITATING & AGGRAVATING FACTORS | PHYSICAL FINDINGS | DIAGNOSTIC STUDIES |
|---|---|---|---|---|---|---|
| Anxiety | Most common cause of palpitations in children and adolescents | — | Sweaty palms, hyperventilation | — | — | — |
| Ingestion of stimulants or drugs (caffeine, alcohol, amphetamines, cocaine) | Patients have decreased tolerance with increased age | — | Nervousness, tremor | Caffeine, alcohol, street drugs | Premature ventricular contractions, tachycardia | Toxicology screening tests |
| Drugs (pseudoephedrine, ACE inhibitors, amphetamines, psychotropic agents, thyroid hormone) | — | — | — | — | Premature ventricular contractions, tachycardia | — |
| Digitalis glycosides | — | — | Nausea, anorexia | Increased digitalis dose, hypokalemia, hypomagnesemia, decreased renal function | PVCs, tachyarrhythmias, bradyarrhythmias, 2° or 3° heart block | Serum digitalis level, ECG, Holter, serum K/Mg/Cr |
| Beta blockers, antihypertensives, calcium channel blockers | Patients with angina or hypertension | — | — | — | Bradycardia | — |
| Hydralazine, minoxidil | — | — | — | — | Sinus tachycardia | — |
| Hypoglycemia | Insulin‑dependent diabetics | Arrhythmias near peak insulin activity | Sweating, headache, tremor, weakness | Increased insulin, decreased carbohydrates | PVCs, tachycardia | Blood glucose |
| Hyperthyroidism | More common in older men | Atrial premature contractions; may be silent | Nervousness, tremors, weight loss | Heart disease | Atrial fibrillation, premature contractions, tachycardias | Thyroid function tests |
| Exercise | Normal; more frequent in CAD, HTN, MVP, cardiomyopathy | — | — | Exercise | — | — |
| Reactive hypoglycemia | — | Recurrent arrhythmias in late afternoon/evening; several hours after carbs | Sweating, tremors, headache, anxiety | — | — | Glucose tolerance test |
| Cardiac Diseases | ||||||
| Mitral valve prolapse | Most common in young women (avg age 38) | — | Sticking chest pain | Exercise | Midsystolic click, late systolic murmur, PVCs/PACs, tachycardia | Echocardiography |
| Wolff‑Parkinson‑White syndrome | Often detected in children/adolescents | Recurrent palpitations; frequent paroxysmal tachycardia | — | Exercise, digitalis | Paroxysmal tachycardia | ECG, Holter |
| Sick sinus syndrome | Older patients | Bradyarrhythmia, tachyarrhythmia | Chest pain, syncope, CHF, dizziness | Exercise, digoxin, beta blockers, CCBs | Bradyarrhythmia, tachyarrhythmia | ECG, Holter, electrophysiologic studies |
| Coronary artery disease | Older patients | Palpitations | Angina, CHF | — | PVCs, paroxysmal atrial fibrillation | Exercise ECG, Holter |
Notes
- How does she describe the palpitations? e.g. skipped heartbeat, irregular heartbeat, rapid/slow heartbeat, increased awareness? A patient’s awareness of the heartbeat occurs most frequently at rest (e.g., while watching television or lying in bed). In bed, the mattress serves as a resonator; this facilitates an awareness of the heartbeat, which may be fast, slow, irregular, or normal.
- All patients should be questioned about the characteristics (fast, slow, irregular, etc.) of the palpitations, mode of onset, mode of termination, precipitating factors, frequency, and results of any prior therapy
- Patients may complain of a forceful, fast, slow, or irregular heartbeat.
- It is often useful to have the patient tap out what the rhythm feels like. If the patient cannot do this, the physician can tap out a selection of rhythms—slow and regular, slow and irregular, fast and regular, and fast and irregular as well as the beat of a premature contraction followed by a compensatory pause—to help the patient describe what he or she means by “palpitations.”
- Are palpitations provoked by exercise/exertion? If the palpitations occur infrequently, are not associated with other symptoms (e.g., chest pain, syncope, dizzy spells), and develop in an otherwise healthy patient, concern or extensive workup is probably unnecessary. If palpitations are frequent, are disturbing to the patient, or are associated with near-syncope or syncope, dizzy spells, chest pain, activity, or evidence of heart disease, they should be considered more serious, and further investigation is required. The studies should include electrocardiography performed with the patient at rest, exercise electrocardiography, and frequent 24-hour Holter monitoring or closed-loop event monitoring.
- Are episodes related to eating or time of day? Various types of arrhythmias are typically found at different times in the same patient.
- Recurrence of arrhythmias in late afternoon and early evening suggests that they are precipitated by reactive hypoglycemia. For any patient with unexplained, recurrent arrhythmias that occur several hours after eating, the physician should perform a glucose tolerance test to rule out reactive hypoglycemia. These arrhythmias are usually supraventricular in origin.
- Arrhythmias in insulin-dependent diabetic patients that occur near the time of peak insulin activity are also frequently induced by hypoglycemia. Patients with diabetes often have accelerated coronary artery disease, which is another possible cause of arrhythmias.
- Does the patient have a history of gastric surgery? Patients who have undergone gastric surgery for obesity may experience palpitations as part of the “dumping syndrome,” which is a constellation of symptoms including nausea, abdominal pain, diarrhea, a sensation of heat, dizziness, reduced blood pressure and palpitations occurring within 15 minutes of ingesting a meal. This is attributable to the rapid transit of food into the small intestine
- Tolerance to caffeine, alcohol, drugs, and other agents decreases with age. These agents, though previously tolerated without symptoms, may induce palpitations as the patient gets older. Palpitations (often paroxysmal atrial fibrillation) are occasionally noted by a patient during the day after unusual but not necessarily excessive alcohol ingestion, a phenomenon known as holiday heart syndrome . The most common causes of palpitations in elderly patients include supraventricular and ventricular premature beats, sick sinus syndrome, and atrial fibrillation.
- Do episodes involve hyperventilation? In anxious patients who complain of palpitations, the arrhythmias may be precipitated by hyperventilation. If this is suspected, the physician can instruct the patient to hyperventilate forcibly for 3 or 4 minutes to determine whether this activity induces an arrhythmia that should be recorded. If signs of hyperthyroidism (resting tachycardia, warm sweaty palms, tremor, exophthalmos, or lid lag) are noted, the arrhythmia may be secondary to hyperthyroidism.
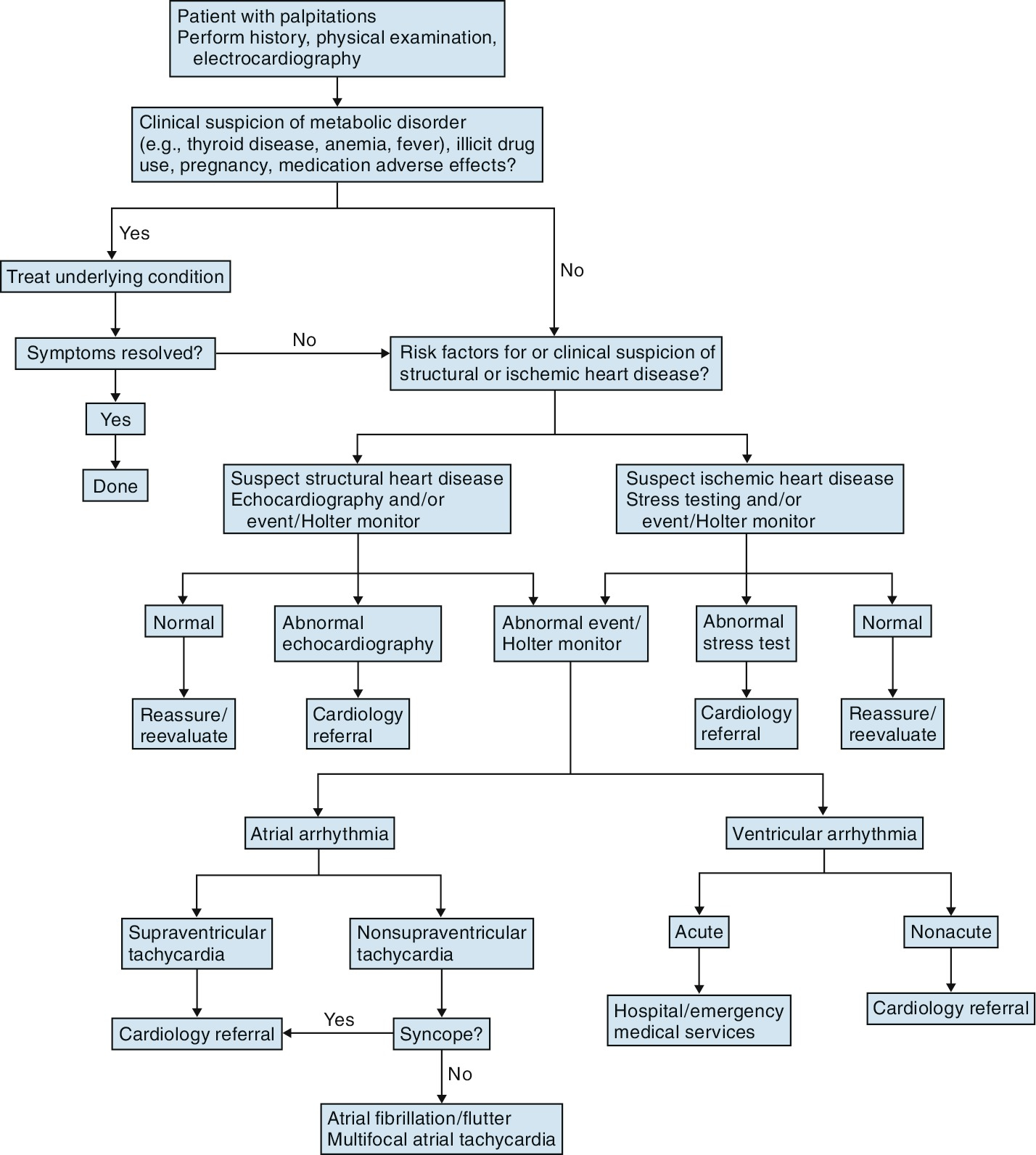
Algorithm for the evaluation and management of palpitations.
2. Chronic nausea and vomiting in a young woman [3]
Chief complaint
Chronic nausea and vomiting for 1.5 years with recent worsening.
HPI
X is a 2x‑year‑old woman presenting to urgent care with a 1.5‑year history of persistent nausea and vomiting, with a notable increase in frequency over the past 3 weeks. Vomiting occurs at least twice daily and consists of small‑volume, watery material with occasional food particles. Episodes are unpredictable and occur during sleep, at work (a sedentary pharmacy job), and throughout the day. During episodes, she is unable to keep down water or food. Vomiting significantly relieves nausea. She has adapted by eating very small amounts throughout the day and has maintained her weight, though she is increasingly concerned about the possibility of weight loss.
- Is there a history of depression? If symptoms of depression are present with little or no weight loss despite a history of long-standing emesis, psychogenic vomiting is probable
- Vomiting usually relieves the symptoms of fullness and pain caused by pyloric obstruction.
- Vomiting relieves nausea if it is being caused by nauseating substances in the stomach. It does not usually alleviate nausea caused by gastroenteritis, gastritis, uremia, or drugs that cause nausea through a central effect.
Her symptoms began around the time she was initially prescribed pantoprazole 40 mg once daily 1.5 years ago. She has continued this medication and, on the advice of her family physician, has increased both the dose and frequency in response to progressive symptom worsening. She denies bilious or bloody emesis, forceful vomiting, abdominal pain, heartburn, chest pain, shortness of breath, headache, vision changes, muscle weakness, bowel habit changes, diarrhea, constipation, urinary frequency, urgency, dysuria, or other urinary symptoms. She reports frequent burping but denies flatulence.
She has had cold symptoms (sore throat and rhinitis) for the past 2 days, but has otherwise been healthy throughout the last 1.5 years. No medications besides pantoprazole and a ansal decongestant (? phenylephrine). No allergies.
Past medical history is significant for schizophrenia.
On review of systems:
- General: no weight loss, fatigue
- GI: chronic nausea/vomiting; no abdominal pain except mild retrosternal aching after vomiting; no diarrhea or constipation; no problem with swallowing
- Acute nausea and vomiting associated with diarrhea and occasionally with abdominal pain are most often caused by gastroenteritis
- Jaundice or hepatomegaly suggests hepatitis or cirrhosis
- CV: no chest pain
- If chest pain or other symptoms of MI are associated with vomiting, the vomiting may be caused by MI. Nausea and vomiting often precede the development of chest pain
- Respiratory: no dyspnea
- Neuro/HEENT: no headaches or visual changes
- Vomiting secondary to increased intracranial pressure (ICP) is often projectile and not preceded by nausea. If headache, ask about postural changes.
- If vertigo and tinnitus are associated with nausea and vomiting, Ménière’s syndrome or disease or other middle ear disturbances should be considered
- When vertigo accompanies vomiting, labyrinthine disorders should be suspected.
- When vomiting without vertigo is induced by a recumbent posture, a posterior fossa lesion should be suspected
- A cloudy sensorium, focal neurologic deficits, or papilledema suggests an intracranial lesion, whereas nystagmus suggests a labyrinthine cause
- GU: no urinary symptoms (hesitancy, dysuria, flank pain, incontinence, frequency, urgency); not sexually active; regular menses
- Hyperemesis gravidarum may cause chronic vomiting during pregnancy. Nausea and vomiting of pregnancy must be considered in women of reproductive age; some pregnant women experience morning sickness in the first trimester of pregnancy, often before they are aware of their pregnancy.
Objective
- General: awake, alert, no respiratory distress; flattened affect
- Vitals: pulse 85 bpm, regular
- Abdominal exam:
- I: Slight distension; no visible peristalsis
- A distended abdomen accompanying nausea and vomiting may indicate paralytic ileus or mechanical obstruction of the intestine
- Abdominal tenderness, distention, and occasionally visible peristalsis suggest GI obstruction
- A: Clear bowel sounds, slightly increased, in all four quadrants
- A succussion splash suggests diabetic gastroparesis
- P: Abdomen is tympanic throughout
- P: Light palpation provokes significant nausea, limiting exam; no reported tenderness; no rigidity or guarding
- No CVA tenderness
- I: Slight distension; no visible peristalsis
Urinalysis reveals 1+ hematuria and WBCs.
Assessment
Chronic nausea and vomiting with preserved weight, watery emesis, nocturnal episodes, tympanic abdomen, and significant aerophagia/burping. No red‑flag symptoms such as hematemesis, severe abdominal pain, or neurologic deficits.
Most likely diagnoses:
- Functional nausea/vomiting given the chronic course, maintained weight, history of schizophrenia, and vomiting that relieves nausea. The fact that vomiting provides relief is characteristic of functional disorders where the act of vomiting reduces visceral hypersensitivity-related nausea.
- Psychogenic vomiting
- Current symptoms of schizophrenia, depression, anxiety?
- History of eating disorders?
- Rumination syndrome remains possible given the small-volume vomiting with food particles and the ability to manage by eating small amounts throughout the day.
- However, classic rumination involves effortless regurgitation within minutes after meals (“meal in, meal out, day in, day out”), which is not clearly described here
- Is it effortless (regurgitation) or forceful (vomiting)?
- Does belching precede regurgitation (rumination)?
- Gastroparesis is less likely given the preserved weight and lack of typical postprandial timing, but cannot be excluded without gastric emptying testing. The small-volume vomiting with food particles could suggest delayed emptying, though patients with gastroparesis typically experience progressive weight loss
- Does vomiting occur immediately during/after eating, 1-2 hours later, or 4+ hours later? This distinguishes functional vomiting (immediate) from obstruction (~2 hours) from gastroparesis (4+ hours).
Critical diagnoses:
| Condition | Supporting Features | Refuting Features | Key Test / Next Step |
|---|---|---|---|
| Antipsychotic withdrawal syndrome |
|
|
|
| Gastric outlet obstruction |
|
|
|
| Pregnancy |
|
|
|
| Metabolic / Endocrine causes |
|
|
|
| Intracranial pathology |
|
|
|
Plan
- Targeted history
- Antipyschotic use: When did she stop antipsychotics? Which medication(s)? Was discontinuation abrupt or tapered? Did symptoms begin during or after discontinuation?
- Timing relationship to meals
- Regurgitation vs vomiting
- Cannabis use (cannabinoid hypermesis syndrome); less likely given continuous pattern and relief from vomiting
- Psychiatric status: current symptoms of schizophrenia, depression, or anxiety? History of eating disorders?
- Focused exam
- Fundoscopy for papilledema
- Sucussion splash test for gastroparesis or obstruction: a stethoscope is placed over the upper abdomen (epigastrium) while the patient is physically rocked back and forth at the hips; indicates presence of excess fluid/gas in dilated stomach
- Abdominal exam when not nauseated
- Labs
- CBC
- TSH
- Urine drug screen (cannabis)
- Upper endocscopy (EGD) is the most important next step - for mechanical obstruction, peptic ulcer disease, mucosal pathology.
- Normal EGD > 4-hour solid-phase gastric emptying scintigraphy to assess for gastroparesis
- Normal EGD and gastric emptying > high-resolution esophageal manometry with impedance for rumination syndrome
- Counselling
- New neurologic symptoms
- Projectile vomiting
- Severe electrolyte imbalance
- Evidence of obstruction
- Treatment
- Functional vomiting = TCAs, esp. if psychiatric comorbidity; CBT; addressing visceral hypersensitivity
- Prokinetics only if gastric emptying is impaired
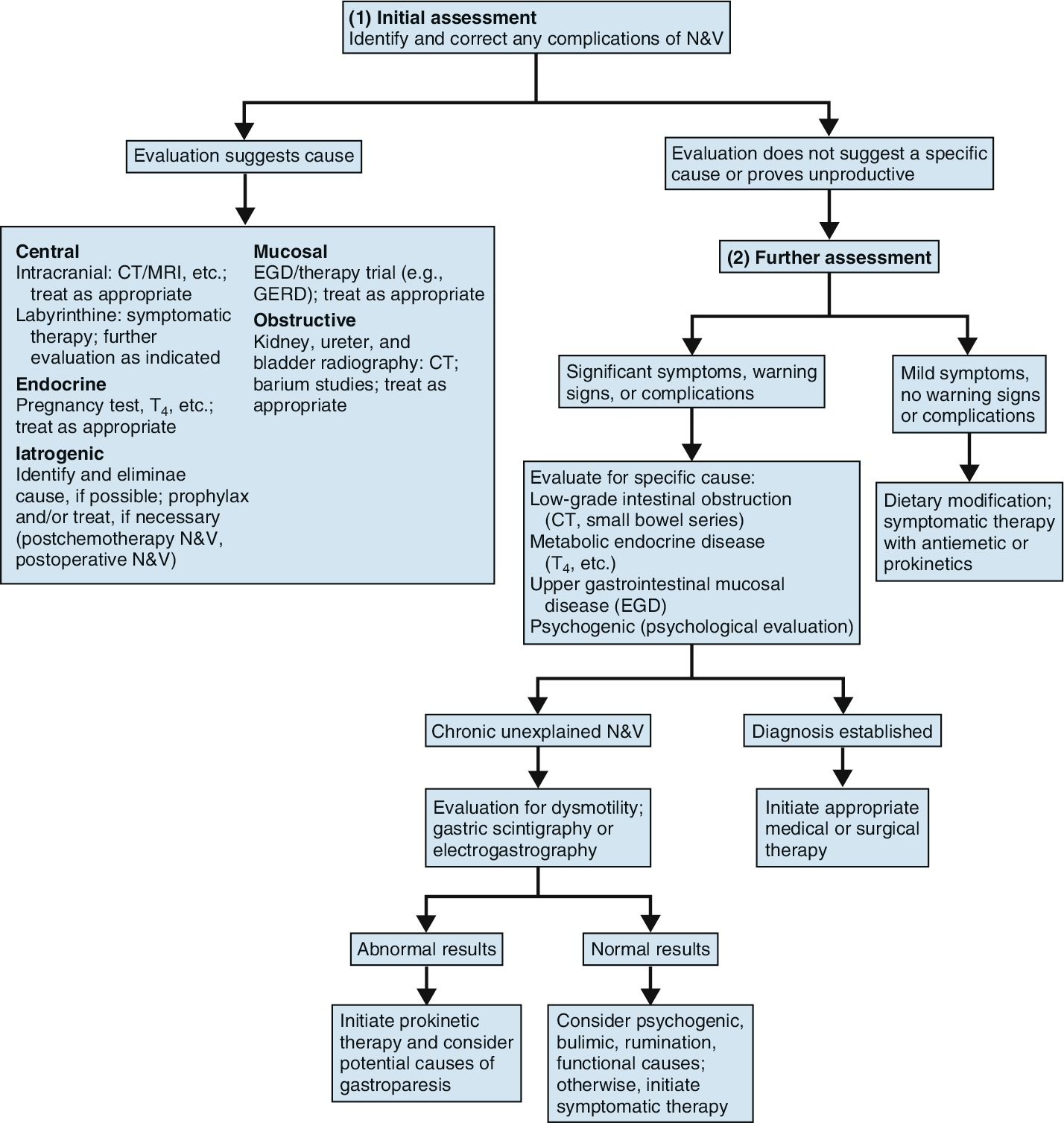
Algorithm for the evaluation of nausea and vomiting
| Cause | Nature of patient | Nature of symptoms | Associated symptoms | Precipitating and aggravating factors | Physical findings | Diagnostic studies |
|---|---|---|---|---|---|---|
| Gastroenteritis | Most common cause at any age | Acute nausea and vomiting | Diarrhea, Fever, Abdominal pain | Hyperactive peristalsis | ||
| Gastritis | Acute or chronic nausea and vomiting occur postprandially | Abdominal pain | Viral infection, Alcohol or drug induced | Endoscopy | ||
| Viral or bacterial infection | Common cause of vomiting in children | Acute nausea and vomiting | Fever | High temperature | ||
| Drugs | Acute or chronic nausea and vomiting | Chemotherapeutic agents, Codeine, Digitalis glycosides, Quinidine, Salicylates, Theophylline, Antihypertensives, Antibiotics | Serum drug level measurements | |||
| Postprandial vomiting | Iron preparations, Proton pump blockers, NSAIDs, Nicotine (including patches, gum) | |||||
| Otitis media | Children | Acute nausea and vomiting | Fever, Earache | Inflamed tympanic membrane | ||
| Excessive alcohol ingestion | Alcoholics, Social drinkers | Early-morning vomiting | Upper endoscopy | |||
| Uremia | Chronic nausea and vomiting, usually early morning | Elevated BUN and creatinine | ||||
| Morning sickness | Pregnant females | Early-morning nausea and vomiting, usually in first trimester | Serum hCG measurement | |||
| Environmental or emotional stresses | Episodic nausea usually without vomiting | |||||
| Diabetic gastroparesis | Diabetics | Succussion splash | Gastric emptying study | |||
| Pyloric obstruction | Infants < 3 months (pyloric stenosis); Adults (ulcer scarring or tumor) | Projectile vomiting | Abdominal pain | Palpable mass, Succussion splash | Ultrasonography | |
| Esophageal obstruction and achalasia | Vomiting/regurgitation of undigested food; odorless vomitus; early morning or after large meals | Esophageal radiograph, Upper endoscopy | ||||
| Increased intracranial pressure | Projectile vomiting not preceded by nausea | Papilledema | Neurologic exam, CSF analysis, CT/MRI | |||
| Pancreatitis | Alcoholics, patients with gallstones | Repeated episodes of unexplained nausea and vomiting | Abdominal pain | Excessive alcohol intake | Elevated serum amylase, CT scan of pancreas |
Notes
- Do episodes occur in clusters, and are there symptom-free intervals? Cyclic vomiting, with or without typical migraine symptoms, may be caused by abdominal migraine, which is more common in children. Cyclic vomiting syndrome is itself an entity characterized by periods of intense vomiting lasting less than a week (three or more episodes per year) with symptom-free intervals in between. It is thought to be related to a mitochondrial DNA mutation and has several triggers, including infection, stress, motion sickness, lack of sleep, menstruation, exhaustion, and certain foods, such as monosodium glutamate, cheese, and chocolate.
- Is there a history of diabetes, or hypoglycemia? Nausea and vomiting can also be the presenting symptoms in patients with hepatitis, myocardial infarction (MI), and diabetic ketoacidosis. Chronic vomiting in adults usually results from gastritis, mechanical obstruction, gut motility disorders (including diabetic gastroparesis ) , achalasia, drugs, labyrinthine disorders, and uremia.
- What are her eating/drinking habits like? Does she use any OTC medications like NSAIDs or Gravol?
- In adults the common causes of acute nausea or vomiting are gastritis (alcohol or drug induced), viral gastroenteritis, psychogenic conditions, and, occasionally, labyrinthine disorders. Common viral pathogens include rotavirus , adenovirus , and norovirus .
- Both food contamination and chemical poisoning must be considered as causes of vomiting, particularly if several people are affected at the same time; in cases of food poisoning, more than one person is usually experiencing symptoms. Toxins from Staphylococcus aureus or Bacillus cereus are often implicated in gastroenteritis from poorly prepared or stored foods.
- Is there a history of psychiatric disorders, esp. eating disorders?
- Self-induced vomiting should be suspected in patients with anxiety, depression, or eating disorders, such as anorexia and bulimia. If these patients are questioned carefully, they may admit to a feeling of nausea, which they attempt to relieve by gagging themselves to produce vomiting.
- Are there any constitutional symptoms or bloody stools?
- If an elderly patient presents with persistent vomiting, gastric or intestinal obstruction secondary to neoplasm should be suspected.
- When vomiting is painless or has preceded abdominal pain by a considerable period, a surgical lesion is unlikely.
- Repeated episodes of unexplained vomiting and nausea may indicate pancreatitis, which is not always associated with abdominal pain.
- Persistent vomiting without any bile staining is an indication of pyloric obstruction. In children this may be caused by pyloric stenosis and, in adults, by ulcer scarring or tumor
- How do symptoms relate to time of day or meals?
- Patients with uremia, pregnant women, and chronic alcoholics often experience early-morning nausea and vomiting.
- Vomiting immediately before food is ingested may be a manifestation of anxiety, depression, or an eating disorder, whereas vomiting shortly after eating may be a consequence of
- gastric outlet obstruction caused by a pyloric channel ulcer, adenocarcinoma, or other infiltrative lesions.
- functional causes, although organic gastric disease should be suspected The Rome III criteria define three separate entities of functional nausea and vomiting: chronic idiopathic nausea, cyclic vomiting syndrome, and functional vomiting
- gastritis
- digitalis toxicity
- Vomiting that begins 20–40 minutes after meals suggests gastric atony associated with diabetes, prior gastric surgery, or peritonitis
- If vomiting begins 1–2 hours after a meal, disease of the biliary tract or pancreas may be the cause.
- In these latter instances, pain is usually not relieved by vomiting
- Recurrent vomiting that occurs 1–4 hours after eating may be due to gastric or duodenal lesions causing gastric outlet obstruction
- Vomiting that follows and relieves an episode of epigastric pain is usually caused by an intragastric lesion or pyloric spasm
- What does the vomitus smell like?
- If the vomitus lacks the pungent odor of gastric acid, a dilated esophagus (possibly from a stricture or achalasia) may be the cause. Patients with this condition frequently vomit in the morning and vomit or regurgitate undigested food.
- If vomitus has a fecal odor, intestinal obstruction or a gastrocolic fistula should be suspected
References
- https://www.clinicalkey.com/student/content/book/3-s2.0-B9780323512329000278#3-s2.0-B9780323512329000278-f27-01-9780323512329?ckSource=search
- https://www.jacc.org/doi/10.1016/j.jacc.2025.05.007
- https://www.clinicalkey.com/student/content/book/3-s2.0-B9780323512329000229